

Mouthwash Was Built on Fear, Not Biology
Why Sterilizing the Mouth Interrupts Signals the Body Relies On

Mouthwash is sold as the final step of “good oral hygiene.” It’s the victory lap after brushing and flossing. The thing you do when you want to feel like you really showed up for yourself in the morning - clean, responsible, a little more put-together than you were five minutes ago.
There’s something comforting about it. The burn, the sharpness, the sense that whatever was lurking has been dealt with. It feels like control. And in a small, ordinary way, it calms a fear most of us don’t articulate: What if I’m not as clean as I think I am?
But the mouth isn’t a countertop you wipe down after a meal. It’s living tissue - highly vascular, deeply innervated, and woven directly into the immune system. It’s also the opening act of digestion, where signals begin moving long before anything reaches the stomach.
It’s home to a microbial ecosystem that does more than keep the breath polite. It helps regulate blood flow, metabolism, and chemical signaling throughout the body. When that ecosystem is repeatedly suppressed, you’re not just “freshening things up.” You’re quieting a system that’s meant to stay active and responsive.
This is the tension worth noticing: we treat the mouth like a surface, when it’s actually a signal hub. We sterilize what was designed to be regulated. So how did we end up here - treating something this alive as if the highest form of care were silence?
Let me tell you.

Mouthwash: A Brief History
Mouthwash feels normal, because it’s been framed as hygiene for over a century. It sits in the same mental category as soap and deodorant - an obvious good, rarely questioned. But it didn’t emerge from a careful study of the mouth as a living system. It came from a particular moment in history, when medicine learned something powerful… and then applied it too broadly.

In the 1860s, British surgeon Joseph Lister demonstrated that antiseptics could dramatically reduce surgical infections. The results were undeniable. Lives were saved. Medicine changed almost overnight.
Out of that success came a simple, compelling idea: If germs cause disease, then killing germs produces health.
In the context of surgery - where open wounds and acute infection were the problem - that logic was exactly right. But it also planted a habit of thinking that would spread far beyond the operating room.

A few years later, an American physician named Joseph Lawrence created an alcohol-based antiseptic and named it “Listerine” - a nod to Lister. It wasn’t designed for daily oral care. It was a general disinfectant.
Early uses included surgical antisepsis, floor cleaning, and even treatment for gonorrhea. The goal wasn’t balance or regulation. It was sterilization.

By the 1890s, the Lambert Company began pitching Listerine to dentists as an oral antiseptic. It worked - somewhat. Dentists were cautious. The benefits were modest. The product stayed respectable, useful… and small.
At this stage, mouthwash was still framed as a tool for specific situations, not a universal ritual.

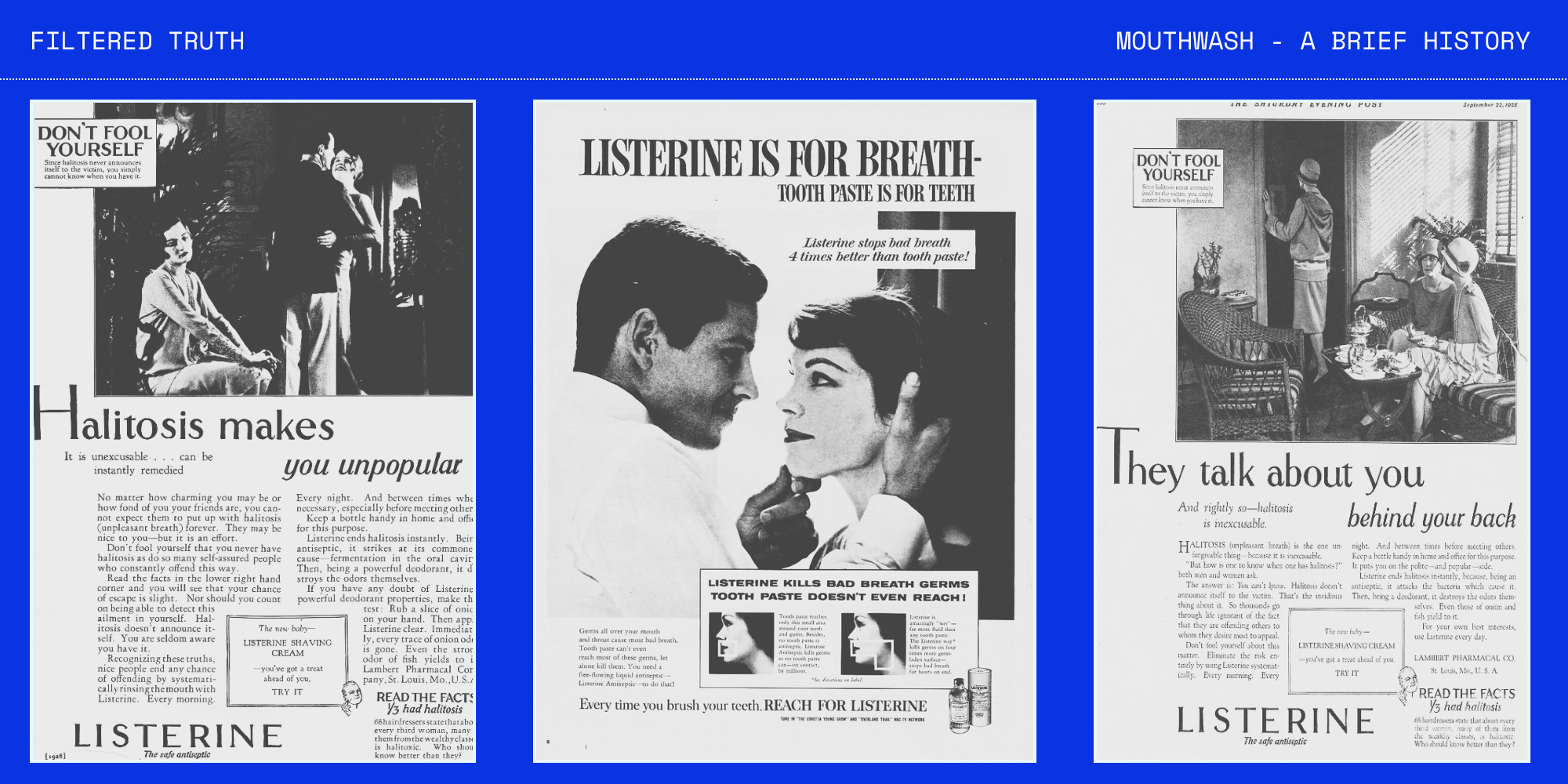
That changed in the 1920s, when Gerard Lambert took Listerine directly to the public and built a national campaign around a newly popularized medical term: halitosis.
The ads didn’t say, “freshen your breath.” They implied something more unsettling:
You are unpleasant.
People are talking about you.
You may never marry...
and only this product can help.
Sales exploded. Mouthwash became a daily habit - not because oral biology had changed, but because the emotional framing had.
First, fear of invisible germs.
Then, fear of social rejection.
Once fear entered the picture, nuance didn’t stand much of a chance.
The problem here wasn’t bad science. It was a narrow idea applied everywhere - one that treated the mouth like a surface to be disinfected, rather than a system to be regulated. And that framing stuck.
The Mouth Is Part of the System
Mouthwash only seems harmless if you imagine the mouth as its own little compartment - a side room you can scrub aggressively without affecting the rest of the house. But that’s not how the body works.
The mouth has a dense blood supply. What touches it touches living tissue. And it sits right at the start of digestion, where inputs move downstream and information loops back upstream. It’s less like a sink you clean and more like a junction - traffic moving in multiple directions at once.
Saliva makes this easier to see.

Saliva is made by glands that pull water and dissolved compounds out of your circulation, then blend them with enzymes, minerals, and protective proteins. In other words, saliva is built from the same internal chemistry that feeds every other organ.
Because of that, it carries a kind of real-time snapshot of what’s happening system-wide - things like:
stress signals (hormone byproducts and metabolites)
nutrient status (what’s being absorbed - or not)
inflammatory chemistry
immune activity
Here’s the part most people never consider:
You don’t make saliva occasionally and spit it out. You swallow it all day.
So whatever shows up in saliva doesn’t stay in the mouth - it’s sent downstream, again and again. This is why treating the mouth like an isolated surface misses the point. It’s not a dead end - it’s part of a circuit:
Blood chemistry builds saliva.
Saliva shapes the oral environment.
You swallow it, sending that chemistry into digestion.
The gut absorbs what it can.
Those compounds re-enter circulation.
Circulation reshapes saliva again.
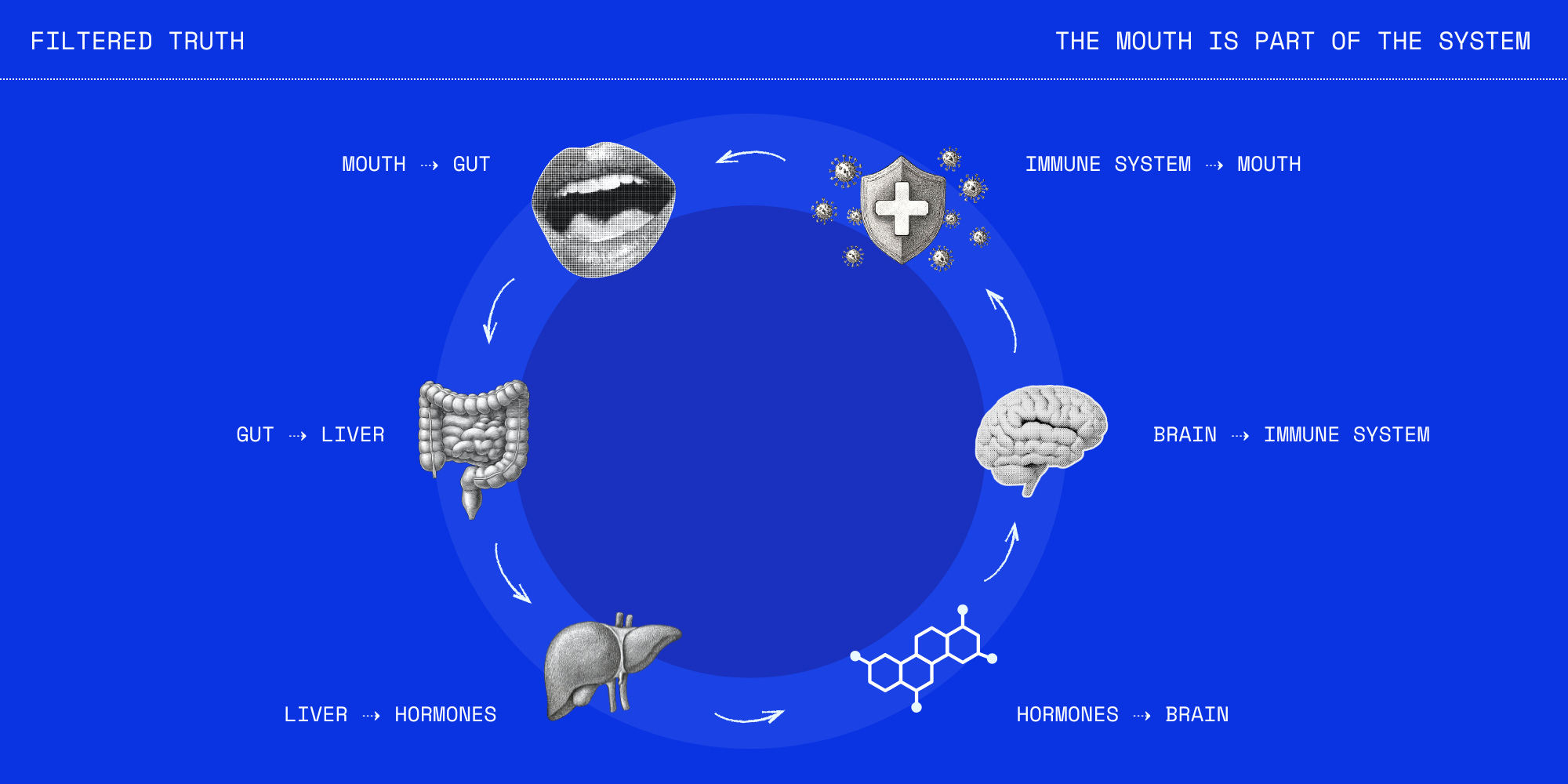
Your oral bacteria aren’t just hanging out on teeth, waiting to cause trouble. They’re integrated into this loop, participating in signaling pathways the body actively relies on. When that ecosystem shifts, the signals shift with it.
What Oral Bacteria Actually Do
If all of this still feels abstract, there’s one simple example where the partnership between the mouth and the body becomes hard to ignore. It involves nitric oxide.
Nitric oxide - often shortened to NO - is a signaling molecule your body uses to manage blood flow. It helps blood vessels relax, supports endothelial function, and plays a real role in blood pressure regulation.
Your body can make some nitric oxide on its own, but one of the most important pathways depends entirely on your oral microbiome. Here’s the basic sequence:
You eat foods that contain nitrates.
Those nitrates enter the bloodstream.
Your salivary glands pull them out and concentrate them into saliva.
Specific oral bacteria convert nitrate (NO₃) into nitrite (NO₂).
You swallow that saliva, and your body converts the nitrite into nitric oxide to support circulation and heart health.
Human cells can’t do this conversion efficiently on their own. Without the right oral bacteria, the pathway stalls - even if your diet is otherwise ideal.
This is one of those quiet partnerships we rarely notice. You feed the system. The bacteria translate the signal. And your physiology benefits downstream.
It’s not contamination. It’s cooperation.
What Gets Broken When We Sterilize
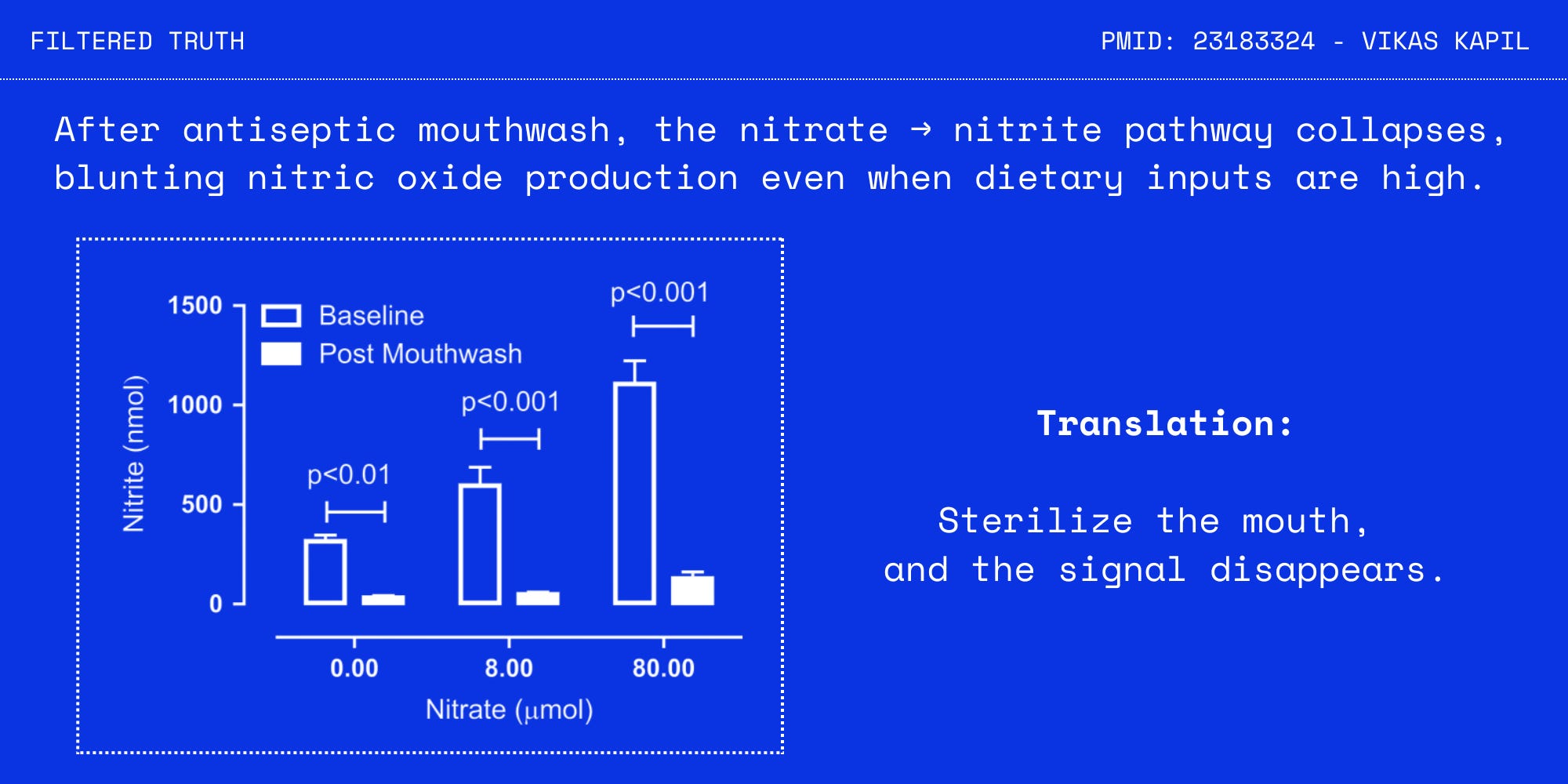
Antiseptic mouthwash isn’t selective. It doesn’t “target bad bacteria.” It suppresses broad groups - including the nitrate-reducing species that make the nitric oxide pathway work. So when you rinse, you don’t just kill germs. You break a link between diet and vascular signaling.
This isn’t hypothetical.
In controlled studies, just one week of twice-daily antiseptic mouthwash reduced nitrite availability and raised systolic blood pressure. In others, suppressing oral bacteria blunted the blood-pressure-lowering effects of nitrate-rich foods - even when people ate the right diet.
Same inputs. Broken processing.
Once you see that, mouthwash stops looking like a harmless cosmetic habit. It starts to look like a daily interruption of a regulatory pathway. So why do we keep using it?
Usually for bad breath. But persistent bad breath is rarely a “dirty mouth” problem. It’s more often a gut problem.
Gut dysbiosis increases fermentation and produces sulfur-based byproducts. Those compounds don’t stay neatly contained in the intestines. They move - via reflux, circulation, and altered saliva chemistry - reshaping the oral environment toward the same odor-producing ecology.
Diet is the primary lever here.
High sugar intake, refined carbohydrates, ultra-processed foods, constant snacking - over time, these keep the system in a fermentative state. Upstream and down. In that context, bad breath isn’t a disease. It’s a signal. And sterilizing signals doesn’t restore balance. It just makes them quieter for a while.
A More Stable Approach
The goal isn’t to sterilize the mouth. It’s to restore the conditions that allow stability.
Start with mechanics, not chemistry. Brush well. Clean between teeth. Remove physical buildup without reaching for daily chemical disinfection. A healthy mouth is regulated, not sterile.
Then look at the terrain. Chronic inflammation, decay, or persistent odor usually point to a body that’s undernourished or metabolically stressed - not a mouth that needs stronger chemicals. What you feed the system matters more than what you rinse away.
Support mineralization from the inside out. Favor nutrient-dense foods that supply the raw materials for repair and resilience: quality animal proteins, eggs, seafood, organs, and mineral-rich traditional foods. Think foundations, not fixes - especially when it comes to fat-soluble nutrients.
If you rinse, keep it simple. Salt water is often enough. The aim is to soothe and support the environment, not flatten it.
Treat persistent bad breath as information. If it lingers despite good hygiene, look upstream. Reflux, fermentation, and gut imbalance are common drivers. Masking the signal may quiet it for a while - but understanding it is what restores balance.
Great post! This makes so much sense!
Excellent post. Thankfully, I’ve never been a regular mouthwash user, probably because I don’t like being “minty fresh.” I don’t like the taste of mint. Good to know what I’ve been doing all my life was the right thing.