

Xylitol: Why I Don't Recommend the "Tooth-Friendly" Sweetener
What the research really says about xylitol, cavities, and whole-body health.

Over the last several issues, we’ve been dissecting the data on fluoride—an additive found in tap water and dental products that quietly interferes with sensitive systems like the thyroid and brain. This week, we are applying that same critical lens to another increasingly popular compound: xylitol.
Marketed as a “tooth-friendly,” “diabetic-safe” sweetener in gum, toothpaste, nasal sprays, and snacks, xylitol is often portrayed as inherently protective. But when you look at how xylitol is made, how it is metabolized, and how it affects organ systems—including the gut, kidneys, and cardiovascular system—a very different picture emerges.
In this issue, we’ll unpack what xylitol actually is, what the strongest research shows, and why I don’t recommend it to my patients.

Contents
What Xylitol Is—and Isn’t
How Modern Xylitol Is Made
How Xylitol Became “Dentist-Approved”
Does Xylitol Actually Prevent Cavities?
Beyond the Mouth: Gut, Kidneys, and Heart
The Bottom Line on Xylitol
Practical Takeaways

Xylitol belongs to a group of compounds called sugar alcohols (polyols). Structurally, it sits between a sugar and an alcohol, which allows it to trigger sweet taste receptors on your tongue while mostly escaping digestion in the upper GI tract. In practical terms, xylitol:
Tastes sweet
Has fewer calories than sucrose
Produces a smaller insulin response than regular sugar
It’s also true that xylitol appears in trace amounts in the fibrous parts of some fruits and vegetables, and that our bodies generate tiny amounts of it as a byproduct of normal glucose metabolism.
But this is where the “natural” story becomes misleading.
The fact that your body makes minute, incidental amounts of xylitol does not mean that large, repeated doses are beneficial - or harmless. And the xylitol added to toothpaste, gum, and “sugar-free” snacks is nothing like a natural plant compound, despite how it’s marketed.

If you’ve heard xylitol referred to as “birch sugar,” you’re hearing a story rooted in its early history. Some of the earliest commercial batches of xylitol were produced from birch wood, which helped create the perception of a clean, Scandinavian, naturally sourced sweetener.
Modern xylitol is very different.
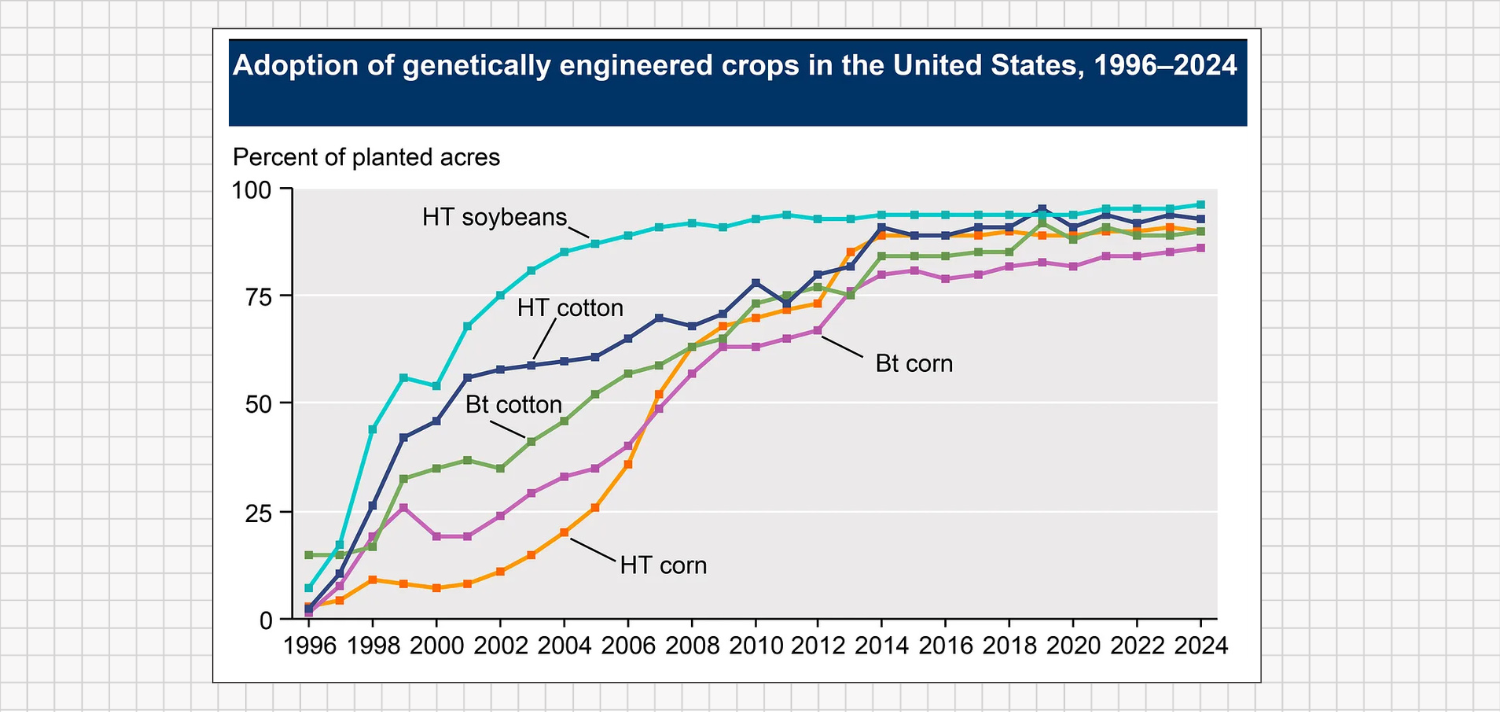
Today, manufacturers typically start with xylan-rich plant waste, most commonly corn cobs or hardwood scraps. In the United States, the cheapest and most abundant source is corn - and because the vast majority of U.S. corn is genetically modified, most industrial xylitol is now largely derived from GMO corn byproducts, not pristine birch forests.
The basic industrial process looks like this:
Acid Hydrolysis: Plant fibers (like corn cobs) are exposed to high heat and sulfuric acid to break down the tough cell walls and release a simple sugar called xylose.
Hydrogenation: The xylose solution is then placed under high-pressure hydrogen gas in the presence of metal catalysts (often Raney nickel). This chemical reaction converts xylose into xylitol.
Purification and Crystallization: The resulting mixture is refined, filtered, decolorized, and crystallized into the bright white powder you see on ingredient labels
From a biological perspective, xylitol is not a nutrient and not a food. It is a refined xenobiotic substance that your body has no evolutionary or physiological requirement for. It does not act as a cofactor for enzymes, does not build or repair tissue, and functions as neither a vitamin nor a mineral. It is simply a laboratory-produced industrial sweetener.

If xylitol isn’t a nutrient and is produced in chemical factories, how did it end up with such a positive, “dentist-approved” reputation?
The story traces back to a period in dental research that was far more focused on targeting specific bacteria than on strengthening the host.
The Turku Sugar Studies
A major part of xylitol’s origin story in dentistry comes from the Turku Sugar Studies conducted in Finland in the 1970s. In these trials, researchers took people eating a typical Western diet and replaced most of their sucrose (table sugar) with either fructose or xylitol for about two years.
At first glance, the results looked impressive: the xylitol group developed far fewer cavities than the sucrose group.
From there, the narrative took off. A nuanced finding quickly hardened into a simple slogan: “Xylitol prevents cavities and is good for your teeth.”
Early dental papers went further, suggesting that xylitol could reduce plaque and support enamel remineralization. Professional organizations later echoed this optimism, and the American Academy of Pediatric Dentistry (AAPD) eventually issued a cautious endorsement of xylitol’s potential to reduce tooth decay in children - more than enough for marketers to roll out bold claims and “dentist-recommended” labels.
The core problem with many of these early trials is that they were never designed to test whether xylitol itself was uniquely protective. They were essentially testing what happens to cavity rates when you dramatically reduce sucrose and replace it with a non-sugar substitute.
In practical terms, participants weren’t just adding xylitol; they were removing a substantial amount of sugar. That makes it very difficult to tell whether any benefit was due to xylitol itself, or simply to eating far less sucrose.

When you look instead at better-designed, longer-term studies - where overall sugar intake is controlled and xylitol is the main variable being manipulated - the apparent benefits become smaller, more inconsistent, and far less impressive than the marketing suggests.
The X-ACT Trial: Nearly Three Years, Minimal Benefit
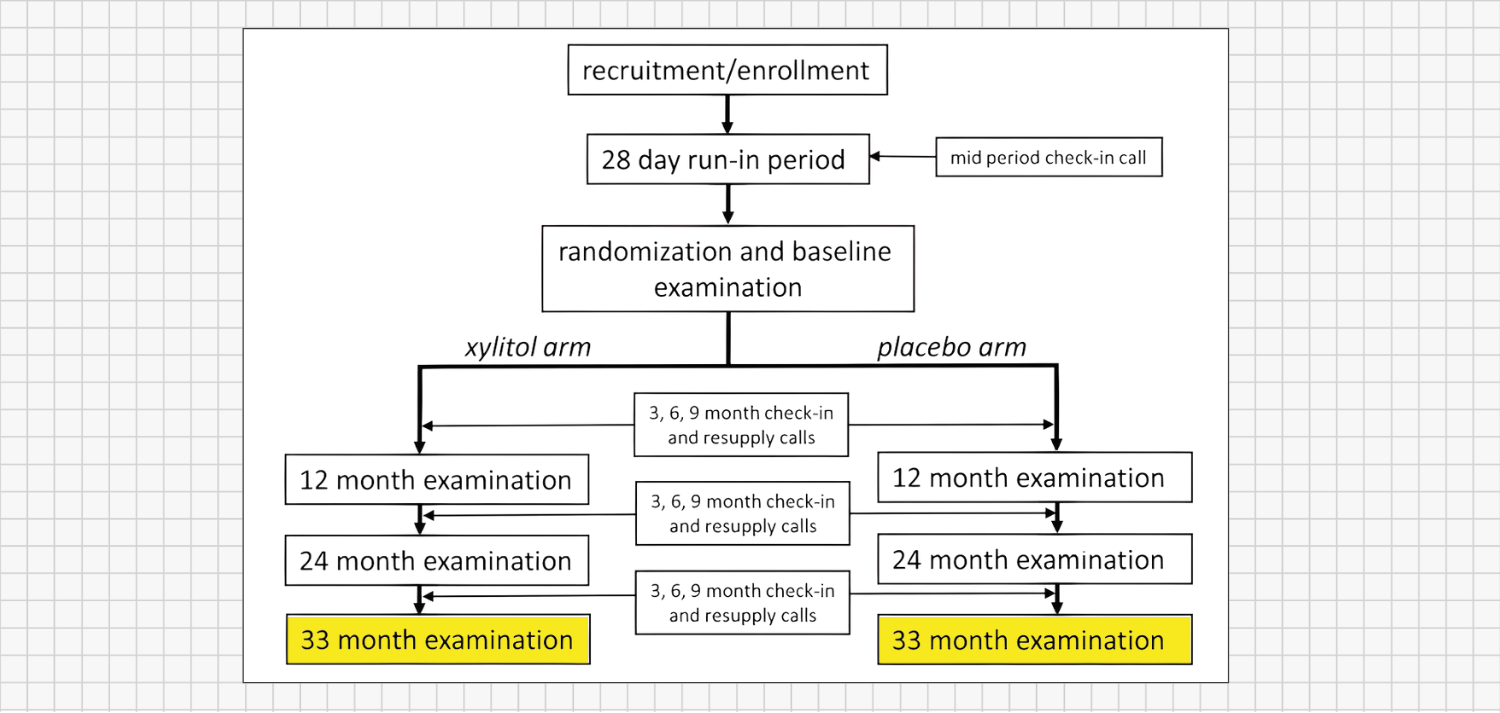
Consider the Xylitol for Adult Caries Trial (X-ACT), one of the most rigorous tests of xylitol’s real-world impact. This was a large, randomized, double-blind, placebo-controlled trial in adults with elevated cavity risk. A total of 691 participants took five 1-gram xylitol lozenges per day (about 5 g total) for 33 months - almost three years - while a control group took placebo lozenges.
The results were underwhelming:
There was about a ~10% reduction in new cavities in the xylitol group compared to placebo.
Quantitatively, this equated to less than one-third of a tooth surface saved per year on average.
This difference was not statistically significant and was considered clinically meaningless.
In other words, after nearly three years of taking xylitol five times a day, there was no clear, meaningful cavity benefit. If xylitol were truly a powerful and reliable anti-cavity agent, a long, well-designed trial like X-ACT should have shown a strong protective effect. It didn’t.
2024 Evidence Review: No Reliable Cavity Protection
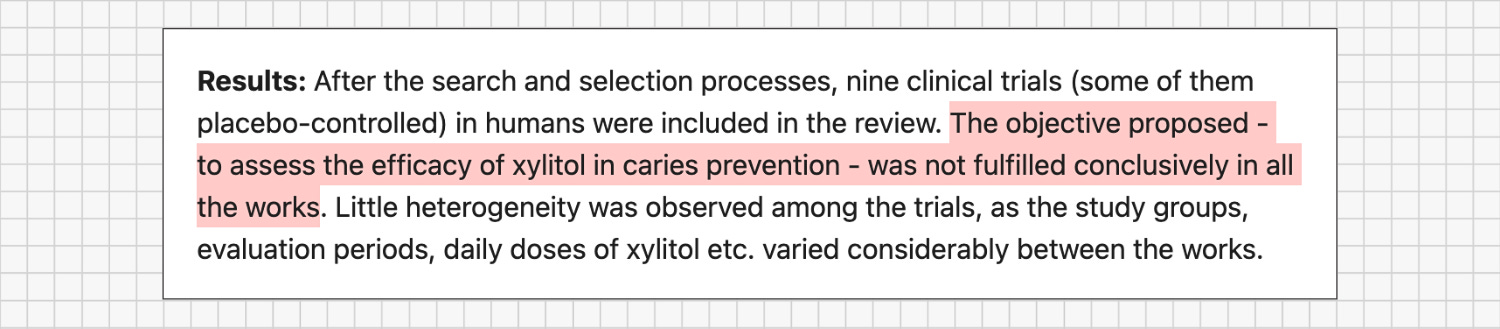
Instead of focusing on a single study, a 2024 systematic review combined data from multiple clinical trials to answer a straightforward question:
Does xylitol consistently prevent cavities?
When the higher-quality studies were analyzed together, xylitol did not emerge as a dependable cavity-prevention tool. The authors ultimately concluded that its preventive effect “cannot be confirmed.”
In plain terms: the popular claim that “xylitol has been proven to prevent cavities” is not supported by strong, consistent evidence.
Gum vs Candy in Children: Chewing vs Xylitol
A 2024 study in children adds another key layer by asking a more nuanced question:
Does the form of xylitol matter?
In this randomized, parallel-group trial, some children were assigned to chew xylitol gum several times per day, while others were given xylitol candies or lozenges containing similar total daily doses. The goal was to see whether chewing versus simply dissolving xylitol in the mouth changed cavity outcomes
The findings were telling:
Xylitol gum was associated with a small reduction in cavities in some children.
Xylitol candies and lozenges showed no meaningful benefit.
Because the total xylitol exposure was similar across groups, the only meaningful difference was chewing (gum) versus not chewing. This strongly suggests that whatever benefit exists likely comes from the mechanical act of chewing, not from xylitol itself.
When you control for sugar intake and look at higher-quality, longer-term trials:
Xylitol does not behave like a robust or consistently effective cavity-prevention agent.
At best, any benefit appears small and highly context-dependent - often tied to the act of chewing rather than xylitol itself.
Overall, the claim that xylitol is a proven, powerful anti-cavity ingredient is not supported by the best available evidence.

Most marketing around xylitol implies that it “stays in the mouth”. But once you chew the gum, swallow the “tooth-friendly” syrup, or brush with xylitol toothpaste, it doesn’t just vanish.
A portion is:
Absorbed (at least partially) in the gut
Processed by the liver and other tissues
Filtered and excreted by the kidneys
In other words, xylitol is not just a local oral ingredient. It becomes a systemic exposure that your gut, kidneys, and cardiovascular system have to deal with.
Let’s look at what we know from human studies and clinical reports
Gut: Osmotic Stress and Microbiome Disruption
The first place xylitol makes its presence known is the digestive tract. Two main issues show up here:
How poorly it’s absorbed
How it reshapes the microbial environment
The mechanism: Your small intestine is designed to rapidly absorb simple sugars like glucose. It is not optimized to handle large amounts of sugar alcohols like xylitol.
Because xylitol is only partially absorbed in the small intestine, a significant portion escapes absorption and travels into the colon.
Once there, the unabsorbed xylitol:
Draws water into the gut (osmotic effect) → loose stools, diarrhea
Becomes fuel for bacteria, which ferment it → gas, bloating, cramping
Study: 2007 High-Dose Xylitol Beverage Trial
In a 2007 randomized controlled trial, adults consumed beverages sweetened with 35-50 grams of xylitol. Compared with sucrose:
The xylitol group experienced significantly higher rates of gas, bloating, and watery diarrhea
In effect, at higher doses, the gut essentially tries to flush xylitol out, confirming its strong osmotic effect.
Review: 2016 Overview of Sugar Alcohols and GI Symptoms
A 2016 scientific review of sugar alcohols found a consistent pattern:
Xylitol and similar compounds cause dose-dependent flatulence, abdominal discomfort, and laxative effects - even in otherwise healthy individuals, and especially in those with irritable bowel syndrome (IBS) or sensitive digestion.
Of course, a pea-sized amount of xylitol in toothpaste is not delivering 35 grams at once. But modern exposure often comes from many small doses throughout the day:
Xylitol gum after meals
Xylitol-containing toothpaste or mouthwash
“Sugar-free” snacks or desserts
A packet of xylitol in coffee or tea
For someone with IBS, chronic bloating, or a sensitive gut, these small but frequent exposures can easily add up to persistent, low-grade gut irritation.
Review: 2019 Polyol Sweeteners and Microbiome Shifts
Beyond immediate GI distress, xylitol can also alter the microbial ecology of the gut.
A 2019 systematic review of polyol sweeteners found that even moderate doses can:
Shift which bacterial species dominate
Alter the pattern of fermentation in the colon
In other words, xylitol is not microbiologically neutral - it actively changes gut flora dynamics.
Given how tightly the microbiome is linked to immune function, inflammation, metabolism, and even mood and cognition, it’s concerning that we have very limited long-term data on what decades of daily xylitol exposure do to the microbiome - especially in infants and children, whose microbial ecosystems are still developing and more vulnerable to disruption.
Takeaway: Xylitol clearly doesn’t just “stay in the mouth”. For many people - especially those with sensitive digestion or existing gut issues - it can add meaningful gastrointestinal stress and change microbiome dynamics in ways we don’t fully understand yet.
Kidneys: Oxalate Load and Filtration Burden
Your kidneys are the body’s main filtration system. They:
Filter blood
Balance electrolytes
Excrete metabolic waste.
Any foreign compound circulating in the blood - including xylitol - eventually reaches the kidneys.
The metabolic pathway: when xylitol is metabolized in the liver, one of its potential downstream byproducts is oxalate. Oxalates are crystalline compounds that can bind to calcium and form calcium-oxalate kidney stones when levels become high enough.
Case Report: 2020 IV Xylitol and Oxalate Nephropathy
We see the potential of this pathway most dramatically in extreme medical use. A 2020 case report in BMC Nephrology described a 39-year-old man who received very large doses of xylitol intravenously.
The outcome was catastrophic:
He developed acute kidney injury and metabolic acidosis.
He eventually fell into a coma.
Kidney biopsy revealed oxalate crystals clogging the renal tubules—the tiny filtration units of the kidneys.
This scenario goes far beyond what you’d encounter from gum or toothpaste. But it proves a key point: xylitol metabolism can generate oxalate, and when that pathway is pushed hard enough, it can seriously damage the kidneys.
Study: 2022 Xylitol Hydration Drinks in Athletes
We also have data from a more relatable context: oral consumption during strenuous exercise.
In 2022, a study in Frontiers in Physiology compared different hydration beverages in semi-professional athletes undergoing strenuous exercise. Drinks were sweetened either with typical sugars (glucose/fructose) or with xylitol. The researchers then measured biomarkers to see how the kidneys and other systems handled the metabolic load.
The xylitol-sweetened drink performed significantly worse across multiple measures:
GI Distress: About 39% of the athletes consuming the xylitol drink developed gastrointestinal issues, including diarrhea. This confirms the osmotic mechanism we discussed earlier.
Blood Markers: The xylitol group showed significant rises in uric acid and creatinine - classic indicators that the kidneys are under increased filtration load.
Urine Markers: There were increases in albumin and cystatin C in the urine, proteins that should mostly be retained, not excreted. Their presence in urine signals acute kidney stress.
The authors concluded that xylitol-sweetened beverages were a poor choice for hydration because they strained the renal system more than regular sugar under these conditions.
Yes, this study was conducted under intense exercise, when kidneys are already working hard. But it underscores a central point:
Xylitol is not an inert passenger in the bloodstream.
It is a compound the kidneys must actively work to process and clear.
Every deliberate “therapeutic” dose (gum, lozenges, powders) adds to this biological filtration burden on your kidneys.
Heart: Platelet Reactivity and Clotting Risk
Perhaps the most striking new data on xylitol comes from the cardiovascular world.
Study: 2024 Xylitol Levels and Cardiovascular Events
For years, non-nutritive sweeteners were assumed to be largely inert once in circulation. A major 2024 study published in the European Heart Journal has fundamentally challenged that assumption.
In this study, researchers measured fasting blood xylitol levels in a large cohort of patients undergoing cardiac evaluation and followed them for three years.
They found:
Individuals with the highest levels of circulating xylitol had a significantly increased risk of major adverse cardiovascular events (MACE) - particularly heart attacks and strokes.
Correlation alone doesn’t prove causation, so the researchers dug deeper.
In a controlled feeding study, participants consumed a xylitol-sweetened drink. The investigators then measured how their platelets behaved and saw:
Platelet reactivity spiked after xylitol consumption.
Platelets became stickier and more prone to clump together.
This creates a pro-thrombotic state, meaning the blood is more inclined to clot. While clotting is essential to stop bleeding after an injury, spontaneous or excessive clotting inside blood vessels is the mechanism behind:
Heart attacks (clots in coronary arteries), and
Ischemic strokes (clots in arteries supplying the brain).
Taken together, these findings suggest that regular xylitol exposure may nudge the body toward a more clot-prone state, especially in those who already have cardiovascular risk factors.

Xylitol is not something the human body is missing. It doesn’t build tissue, support growth, or participate in any essential role in human physiology. It’s a lab-refined sweetener made from industrial plant waste and added to “oral health” products because it fits a convenient marketing narrative - not because our bodies require it.
When you take in a substance your body doesn’t actually need - like xylitol - it still has to be handled by your organs. It must be broken down, moved through the bloodstream, processed by the liver, and filtered by the kidneys. If this happens several times a day, year after year, that extra processing adds to the load on systems that are already burdened with modern diets and environmental exposures. Over time, the accumulated stress can wear these systems down and increase long-term health risks.
At the same time, xylitol doesn’t address the real problem it’s marketed to fix. Cavities and oral disease are not caused by a xylitol deficiency; they’re the predictable result of an undernourished, overburdened system - under-mineralized teeth and bones, compromised jaw and airway development, weak saliva, and daily habits that chronically stress the body. Chewing something that happens to contain xylitol may offer a small, indirect benefit through saliva stimulation, but it does nothing to rebuild that missing foundation.
From that lens, building a prevention strategy around a synthetic sweetener doesn’t make sense. If our aim is true prevention - for ourselves and especially for our children - a more honest approach is to remove as many unnecessary synthetic inputs as we can, including daily xylitol, and focus on what human physiology has always depended on: mineral-rich, nutrient-dense whole foods; robust fat-soluble vitamin and mineral status; healthy breathing and chewing patterns; and clean, non-disruptive oral care products. When those pieces are in place, we don’t need xylitol to “rescue” our teeth—we’re supporting the system that keeps them healthy in the first place.
Practical Takeaways
To put all of this into daily life, here are the key points to remember:
Don’t treat xylitol like a nutrient or a health supplement.
Your body doesn’t need xylitol for anything. It’s a non-essential, industrial sweetener - not a missing dietary building block. Xylitol may offer a little sweetness with fewer calories, but it’s not a health-boosting ingredient, and its cavity-fighting power is modest and inconsistent at best.Be cautious with daily “therapeutic” use.
An occasional piece of xylitol-sweetened gum is one thing. But if you’re deliberately using xylitol after every meal (gum, mints, candies) or adding xylitol syrup/powder to foods “for your teeth,” remember this isn’t the same as taking a vitamin. Any cavity benefit is minor, and high habitual use might quietly stress your gut, kidneys, cardiovascular system, or metabolism over time. In short: don’t overdo it or treat xylitol like a must-have dental routine.Put your effort where the payoff is biggest: nutrients and structure.
Focus on what truly rebuilds and protects teeth and jaws - especially if you’re planning a pregnancy, are currently pregnant, or raising young children. Prioritize:Nutrient-dense foods rich in vitamins A, D, and K₂ (egg yolks, grass-fed butter, organ meats, oily fish, fish eggs).
Mineral-rich foods (quality dairy, bone broths, read meat, organ extracts, mineral-rich stocks).
Adequate protein from well-raised animal sources (meat, poultry, seafood).
Real chewing of fibrous, whole foods to support jaw development and saliva flow.
This is where real, long-term cavity prevention happens. Strengthen the body and the teeth from the inside out, and you naturally become less prone to decay.
You don’t need to micromanage every ingredient label or swear off all sweet tastes to improve your dental health. But when it comes to xylitol, it’s useful to view it through a whole-body, nutrition-first lens.
In the end, strong teeth come from nourishment, not novelty.
Thanks for clarifying the effects of xylitol, because I thought this was a good sugar substitute.
Thanks for reading, I’m glad it was helpful. When something is marketed as a healthier substitute, it’s natural to trust it. My goal is just to fill in the parts that usually get left out